Article page checkbox is not checked in page info.
World Health Organization at a crossroads
World Health Organization at a crossroads
Gabija Leclerc, Members' Research Service

Summary
The World Health Organization (WHO) has had a central role in numerous health advances, including eradicating smallpox, driving the near‑eradication of polio, expanding childhood immunisation worldwide, and leading responses to global health threats such as HIV/AIDS and COVID‑19. Despite this, the United Nations (UN) specialised agency has faced persistent challenges, shortcomings and criticisms over decades. The agency has been limited by volatile, insufficient and distorted funding. Its complex governance and limited authority, compounded by political pressure, also compromise the agency's ability to carry out its mandate effectively. In addition, misinformation and disinformation have been obstructing the WHO's action. To address its systemic weaknesses and increase its capacity to overcome evolving challenges, the WHO launched its Transformation Agenda – an ambitious organisational change plan – in 2017.
Although the WHO has successfully implemented many actions under its Transformation Agenda, owing to persistent structural weaknesses and newly arising challenges, the agency is still at a critical juncture. The second half of the 2020s is especially difficult for the agency. Following the United States' (US) withdrawal from the WHO, which was initiated in January 2025 and precipitated a sudden US$1.3 billion shortfall, 25 % staff reductions, loss of expertise and programme suspensions, historical vulnerabilities are now amplified to unprecedented levels. Moreover, declining investments in development assistance, including its health component, further intensify the financial pressure.
The EU and the WHO enjoy a long-lasting strategic partnership. The EU supports the WHO's Transformation Agenda and contributes to a wide range of WHO programmes, focusing on areas such as UHC, strengthening health systems worldwide, health security, antimicrobial resistance, and enhancing laboratory capacities in Africa.
Through its resolutions, the European Parliament has repeatedly expressed its strong support for the agency and called on the Commission and the EU Member States to comply with different WHO measures, initiatives and guidelines. Parliament supports the EU in seeking official observer status at the WHO.
Introduction to the World Health Organization
Established in 1948, the World Health Organization (WHO) is the United Nations (UN) specialised agency working with almost 200 countries on efforts to expand universal health coverage (UHC), promote healthier lives, and coordinate the response to health emergencies. As per its Constitution, the WHO's key objective is 'the attainment by all peoples of the highest possible level of health'. To achieve this, the agency acts as 'the directing and coordinating authority on international health work'.
WHO's mandate
According to the WHO Constitution, the agency's functions include:
-
acting as the directing and co-ordinating authority on international health work;
-
fostering collaboration with relevant actors;
-
assisting governments, on request, in strengthening health services;
-
providing technical assistance and, in emergencies, necessary aid;
-
providing administrative and technical services as required, including epidemiological and statistical services;
-
promoting and conducting research in health, and promoting co-operation among scientific and professional groups;
-
providing information, counselling and assistance in the field of health;
-
establishing and revising international nomenclatures of diseases, of causes of death and of public health practices;
-
standardising diagnostic procedures;
-
developing, establishing and promoting international standards with respect to food, biological, pharmaceutical and similar products;
-
proposing conventions, agreements and regulations, and making recommendations on international health matters;
-
taking all necessary action to attain the agency's objective.
The WHO Constitution prescribes the agency to work in the following key areas:
-
epidemic, endemic and other diseases;
-
prevention of accidental injuries;
-
nutrition, housing, sanitation, recreation, economic or working conditions and other aspects of environmental hygiene;
-
maternal and child health and welfare;
-
mental health.
The agency's highest decision-making body is the World Health Assembly (WHA), composed of delegates representing WHO member states, which meets at least yearly to adopt conventions, agreements, regulations and recommendations on any matter within the WHO's competence or relating to its operations. Currently, all EU Member States are WHO members; the EU itself is an unofficial observer.
The WHO has been central in numerous health advances, including eradicating smallpox, driving the near‑eradication of polio, expanding childhood immunisation worldwide, and leading major responses to global health threats such as HIV/AIDS and the COVID‑19 pandemic. The agency has also been instrumental in developing norms and standards, including the legally binding WHO Framework Convention on Tobacco Control (FCTC), the International Health Regulations (IHR) and the WHO Pandemic Agreement, as well as essential medicines lists, and disease classifications used worldwide.
Throughout the decades, the WHO's scope of action expanded from infectious disease control to encompass non-communicable diseases (NCDs), UHC, pandemic preparedness and beyond. Under the Fourteenth General Programme of Work 2025–2028 (GPW 14), the agency centres its work on six strategic objectives: (i) respond to climate change; (ii) address health determinants and the root causes of ill health in key policies across sectors; (iii) advance the primary healthcare approach and essential health system capacities for UHC; (iv) improve health service coverage and financial protection to address inequity and gender inequalities; (v) prevent, mitigate and prepare for risks to health from all hazards; and (vi) rapidly detect and sustain an effective response to all health emergencies. Moreover, the key focus of the GPW 14 is also on powering the global health agenda and optimising the WHO's performance.
Key WHO challenges
Although the WHO is instrumental in international global health cooperation, the agency has faced persistent challenges, shortcomings and criticisms over the decades. These often pertain to (i) volatile, insufficient and distorted funding; (ii) complicated governance, limited authority and political pressure; and (iii) vulnerability to misinformation and disinformation. The second half of the 2020s seems to be particularly difficult for the WHO, with all the challenges and vulnerabilities requiring urgent solutions to ensure the agency can continue to function.
Funding
Financing gap
The WHO has long been struggling with chronically insufficient funding. The progressive expansion of its mandate amid stagnant financing forced the agency to confront difficult prioritisation decisions and trade-offs across programmes. Yet, the financing situation has never been as difficult as following the United States (US) withdrawal from WHO, initiated in January 2025 and concluded one year later, which precipitated a sudden US$1.3 billion shortfall (18 % of prior budget), 25 % staff reductions, and programme suspensions – amplifying historical vulnerabilities to unprecedented levels. Moreover, declining investment in development assistance, not least in its health component, observed worldwide, including in Europe, make the financial pressure even more acute.
US withdrawal
The US has been a member of WHO since 1948. The US financial contribution – the largest globally – has been vital to the WHO. The US supported the agency through assessed (core, or mandatory) contributions, set at 22 % of the WHO core budget (US$134.58 million, or around €114.63 million for 2025), as well as voluntary contributions with an average annual amount of US$237 million (or almost €202 million) between 2012 and 2024. In terms of overall funding – voluntary and mandatory – the US contribution amounted to between 16 % and 18 % of the total WHO budget, depending on the year. On 20 January 2025, on his return to the White House, US President Donald Trump initiated the US withdrawal from WHO through an executive order. 1 The executive order accused WHO of continuing to demand 'unfairly onerous payments ... far out of proportion' with other countries' assessed contributions – annual amounts that each of WHO member and associate member is required to pay to WHO. In particular, the executive order pointed at China, which, with a population of 1.4 billion – around 4.3 times larger than the US population – allegedly 'contributed nearly 90 % less to WHO' than the US. In reality, whereas the US paid a 22 % share of the WHO core budget, China was asked to pay almost 15.3 %, and the 27 EU Member States together contributed almost 24 % in the fiscal year 2024-2025 (see Figure 1).
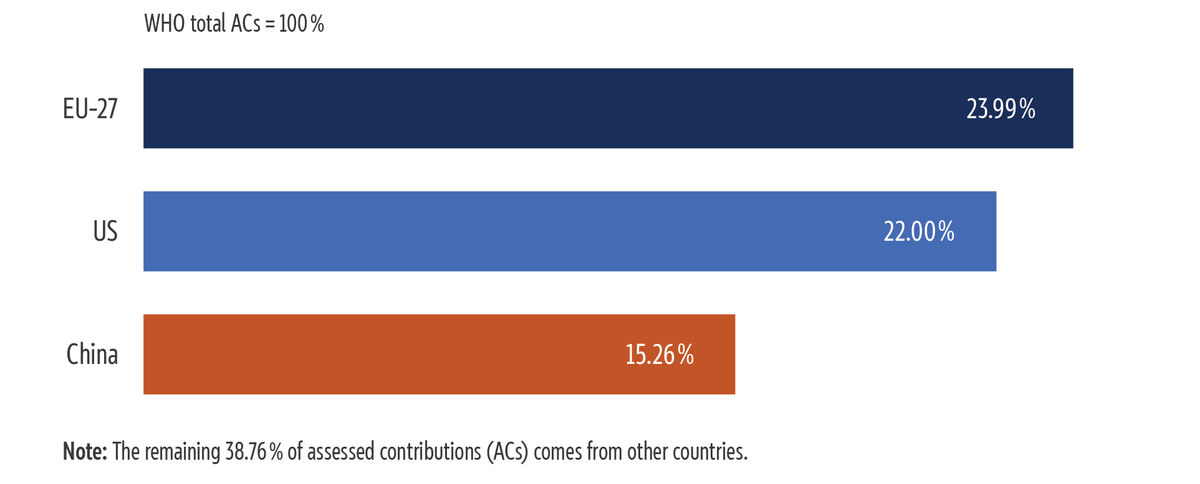
Source: Compiled by the author based on WHO data. Graphic by Nadejda Kresnichka-Nikolchova, EPRS.
Regarding the overall contribution to the WHO budget, in the years 2022 to 2023, the US contribution of US$1.28 billion (around €1.09 billion) amounted to 16.2 % of the total WHO budget; China provided the WHO with US$0.16 billion (around €0.14 billion), accounting for 2 % of the total budget. Meanwhile, the contributions from the European Commission, the EU Member States and the European Investment Bank (EIB) amounted to US$2.35 billion (€2 billion), or 29.8 % of the total 2022-2023 WHO budget (see Figure 2).
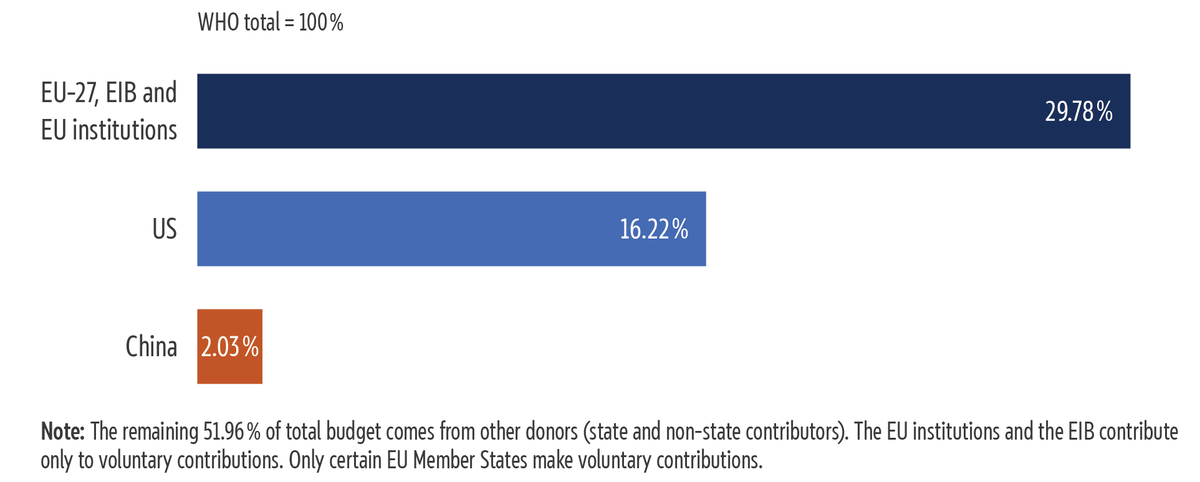
Source: Compiled by the author, based on WHO data. Graphic by Nadejda Kresnichka-Nikolchova, EPRS.
The impact of the US withdrawal is broader than the stark financial loss. It also resulted in the loss of human resources and technical and scientific expertise, among other things. The withdrawal also reduces the WHO's quasi-global reach and creates new challenges in an even more fragmented global health landscape (see the section 'Governance, authority and political pressure' below).
In this context, the WHO was forced to accept a 9 % decrease in its budget for the years 2026 to 2027 compared with the budget agreed for the previous biennium (see the Table 1). As a result, WHO's 2026-2027 programme budget totals US$6.2 billion – US$0.6 billion less than in the years 2024 to 2025 and US$1.2 billion less than initially proposed by the WHO Executive Board (EB)2 for the years 2026 to 2027. This budget covers base programmes, which represent the WHO's core mandate and the largest part of its budget (US$4.27 billion); polio eradication (US$770.9 million);3 special programmes (US$168.7 million);4 as well as emergencies and emergency appeals (US$1 billion).5
| Budget segment | Programme budget 2020-2021 | Programme budget 2022-2023 | Programme budget 2024-2025 (1) |
| Base programmes | 3 768.7 | 4 968.4 | 4 968.2 |
|---|---|---|---|
| Polio eradication | 863.0 | 558.3 | 694.3 |
| Special programmes | 208.7 | 199.7 | 171.7 |
| Emergency operations and appeals | 1 000.0 | 1 000.0 | 1 000.0 |
| Total | 5 840.4 | 6 726.4 | 6 834.2 |
Data source: WHO, Proposed programme budget 2026-2027, 2025. Note: RC: regional committees; EC: Executive Committee; WHA: World Health Assembly.
| Budget segment | Proposed programme budget 2026‑2027 (RC version) | Proposed programme budget 2026‑2027 (EB version) | Programme budget 2026‑2027 (adopted by WHA) (2) | Difference between (1, previous table) and (2, this table) |
| Base programmes | 5 687.7 | 5 324.1 | 4 267.1 | -701.1 |
|---|---|---|---|---|
| Polio eradication | 976.3 | 976.3 | 770.9 | +76.6 |
| Special programmes | 172.8 | 172.8 | 168.7 | -3.0 |
| Emergency operations and appeals | 1 000.0 | 1 000.0 | 1 000.0 | 0.0 |
| Total | 7 836.8 | 7 473.2 | 6 206.7 | -627.5 |
Data source: WHO, Proposed programme budget 2026-2027, 2025. Note: RC: regional committees; EC: Executive Committee; WHA: World Health Assembly.
Inflexibility
WHO also struggles with a lack of flexibility in using its funds. The agency is funded through two primary sources: assessed contributions from member states and voluntary contributions from partners (see Figure 3).
Assessed contributions, i.e. mandatory dues based mainly on a country's gross domestic product and adjusted for WHO's membership, are a key source of financing for WHO, providing predictable and flexible financing. They are approved by the member states every two years at the World Health Assembly. Before 2022, they accounted for less than 20 % of the WHO programme budget. However, after increases in May 2023 and May 2025, the assessed contributions now cover around 40 % of the WHO budget, with a target of 50 % by 2030.
Voluntary contributions from governments, UN agencies, foundations and private donors make up the remaining 60 %. These fall into three categories based on flexibility:
-
core voluntary contributions (fully flexible);
-
thematic and strategic engagement funds (partially flexible);
-
specified voluntary contributions (inflexible, tightly earmarked for specific programmes; account for more than 85 % of the total voluntary funds).
As a result, a big part of WHO funds is not flexible. This limits the WHO's discretion in deciding on its action, and is often seen as limiting the agency's agility in carrying out its mandate. In particular, it results in a prioritisation mismatch when the WHO is obliged to adhere to the donor priorities – such as health security – over other needs, such as addressing the determinants of health or ensuring equitable access to medicines. Inflexible funding also slows down adaptation, which is particularly visible during major crises such as COVID‑19, when the agency struggled with the timely repurposing of funds. Finally, some note that a few powerful donors are able of shaping the WHO's action, which again limits the agency's autonomy and discretion.
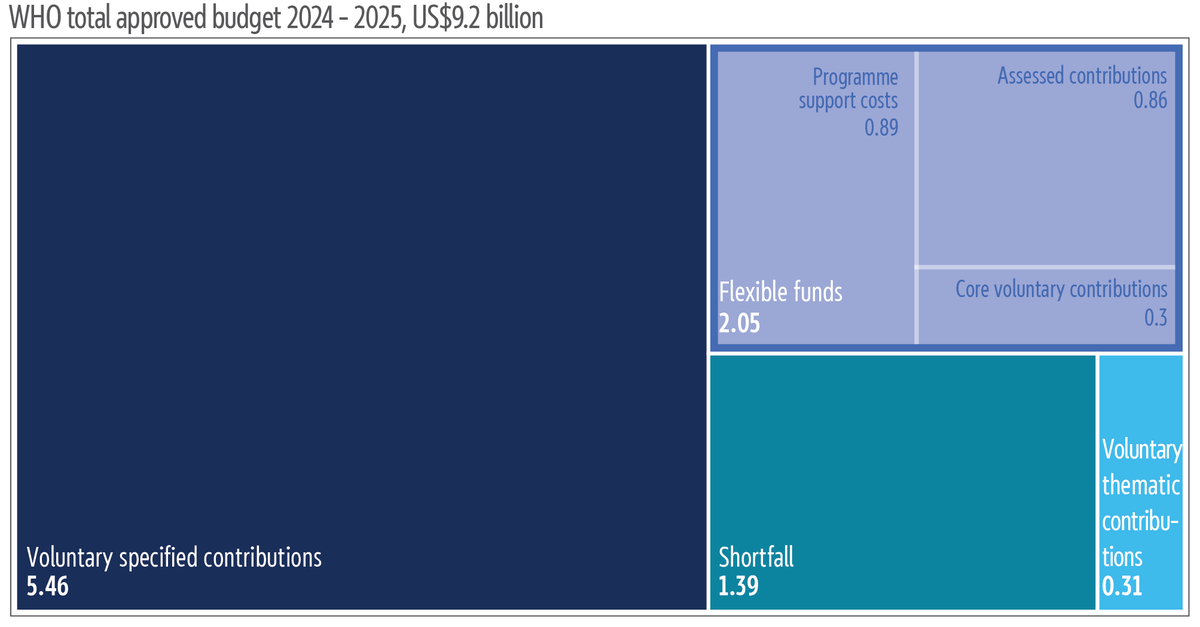
Source: Compiled by the author, based on WHO data. Graphic by Nadejda Kresnichka-Nikolchova, EPRS.
Unpredictability
In addition to being insufficient and inflexible, the WHO's funding is characterised by unpredictability. Most of the agency's funds are voluntary contributions with no guarantee of timely payment or renewal. This undermines the WHO's ability in the long-term planning of its actions, particularly those that are not on the top of key donors' agenda (e.g. the burden of NCDs; occupational health and safety, UHC). This often results in the agency having a reactive, short-term focus. Moreover, the WHO is susceptible to facing programme disruptions owing to late, reduced or stopped pledges. For instance, because of the US withdrawal from the WHO and an overall decline in global health financing, the agency experienced an immediate financial hit that resulted in serious operational disruptions, including workforce cuts, programme halts and other operational difficulties pertaining, among other factors, to the urgent need for reprioritisation (see text box below).
Reprioritisation efforts
Following the announcement of the US withdrawal from the WHO and rapidly decreasing global health funding worldwide, both of which resulted in a reduced financial envelope for the WHO, the agency launched a reprioritisation and realignment process. This is grounded in the principle that the WHO should focus its efforts where it provides the greatest added value. The preliminary results show that the agency should (i) refocus on its core mandate stipulated in the WHO Constitution – leadership, policy options, norms and standards, research, monitoring and technical support; (ii) better delineate work from partners and WHO member states; (iii) seek better alignment across the WHO's three levels; and (iv) consolidate fragmented efforts and address duplication.
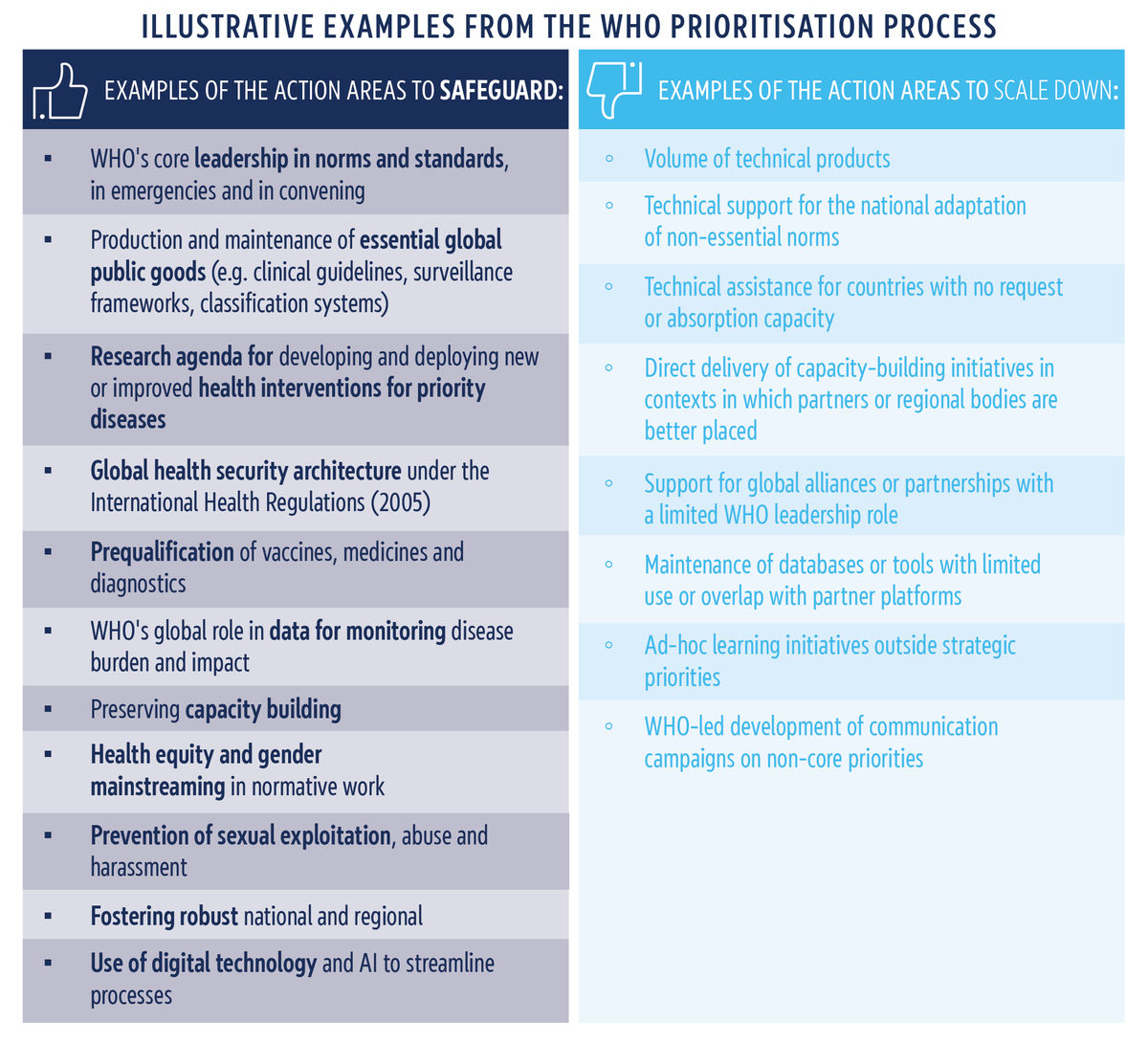
Source: Compiled by the author, based on WHO data. Graphic by Nadejda Kresnichka-Nikolchova, EPRS.
Governance, authority and political pressure
The WHO is challenged, among other things, by its governance, owing to disagreements about the agency's purpose, limited authority due to insufficient independence and legal power; and political and funding pressure from member states.
First, WHO operates in a highly fragmented global health landscape with many different actors at the regional, national and local levels. Over the decades, the field of global health has become increasingly crowded. Global health actors include not only the WHO and its member states (with health actors at different levels) but also international organisations such as the World Bank, which branched out into funding health projects in the 1980s; public-private partnerships such as the GAVI Vaccine Alliance; private foundations such as the Bill Gates Foundation; and non-governmental organisations such as Médecins Sans Frontières. In 2026, following the US and Argentina's withdrawal notifications and their efforts to replace WHO-led global health effort with bilateral partnerships, fragmentation has further increased. This is seen both as challenging the WHO's authority as the main global health actor globally and its visibility. Moreover, with many global health actors having divergent interests and priorities, the WHO has to navigate in a complex, highly nationalised and politicised global health environment.
Second, the agency itself relies on regionalisation of its offices. Currently, WHO member states belong to six regions: the Americas, Europe, the Eastern Mediterranean, South-East Asia, the Western Pacific and Africa. The regions have a high level of autonomy with their own leadership, budget and priorities. Some experts go as far as to argue that the WHO functions not as a single organisation but as seven separate ones – the six regional offices along with the headquarters. While the regional offices are important to adapt global health priorities to suit local context, some experts note that the WHO regional offices structure often hinders global coherence, coordination and the WHO's effectiveness in addressing global health issues. For instance, during health crises, this regionalisation has been shown to obstruct the fair distribution of resources. During COVID‑19, in particular, studies reported inequitable vaccine distribution (via COVAX) and inconsistencies in pandemic responses, partly due to regional offices focusing on local national interests rather than global solidarity.
These structural challenges – fragmentation of the global health landscape and a heavy regionalisation of the agency itself – lower the WHO's ability to effectively carry out its mandate. Most notably, analysts argue that the WHO struggles with ensuring efficient coordination between actors, maintaining its relevance and visibility among proliferating global health actors, including non-governmental ones, and navigating between the diverging interests of its member states and regions. That said, divergent interests and power dynamics among WHO member states mean decisions in the World Health Assembly and Executive Board often reflect politics and bargaining instead of purely technical public health priorities. Moreover, due to its reliance on funding from a few key actors – either member states or non-county contributors – the agency is forced to focus on actions that are aligned with those contributors' interests.
Experts also argue that the agency is not equipped with the necessary authority for its mission, because global health governance requires extensive oversight and enforcement powers (e.g. to verify data, inspect sites or sanction non‑compliance) that the WHO does not have. To give an example, the International Health Regulations, adopted under WHO auspices, are legally binding but heavily depend on national reporting and compliance; without sanctioning and overall enforcement power, the WHO often struggles to compel governments to share timely, accurate information or to implement its measures and recommendations. This results in the WHO relying on technical cooperation instead of stronger measures and their enforcement, which in turn is seen as a limitation to the agency's authority and efficiency, particularly during emergencies. Most notably, during the COVID‑19 pandemic, the WHO was criticised for being too deferential to China and slow to challenge its early handling of the outbreak, reflecting a non‑confrontational strategy that collided with a highly politicised environment.
Vulnerability to misinformation and disinformation
The WHO is facing additional challenges – misinformation and disinformation – that constitute obstacles to effectively carrying out the agency's mandate. This is because misinformation and disinformation negatively affect people's health behaviours and erode trust in the WHO. A paper published in the Bulletin of the World Health Organisation in 2022 found that poor-quality health-related information, misinformation and disinformation is present, in particular, during pandemics, humanitarian crises and health emergencies at an increasing rate. This is problematic in that such spreading of misinformation or disinformation in crisis situations often amplifies vaccine hesitancy and promotes unproven – and sometimes harmful – treatments, as well as non-compliance with official guidance and measures. Moreover, more recently, the negotiations on the WHO Pandemic Agreement were challenged with misinformation and disinformation, fuelling opposition to the initiative. WHO officials claimed that conspiracy theories and false claims, including those arguing that the agreement would take away sovereignty from countries by imposing lockdowns or vaccine mandates, were responsible for an increase in public opposition to the agreement and for hindering negotiations.
Recognising this increasing challenge, WHO has taken several steps to counter misinformation and disinformation and increase resilience to them. The WHO now runs infodemic management activities, including monitoring of social and news media, network analysis of misinformation ecosystems, and coordination with a large network of fact‑checking groups. For example, WHO worked with YouTube to enhance its COVID-19 misinformation policy and provide guidelines for content providers to ensure no medical misinformation relating to the virus proliferates on their platform.
WHO's transformation to address the challenges identified
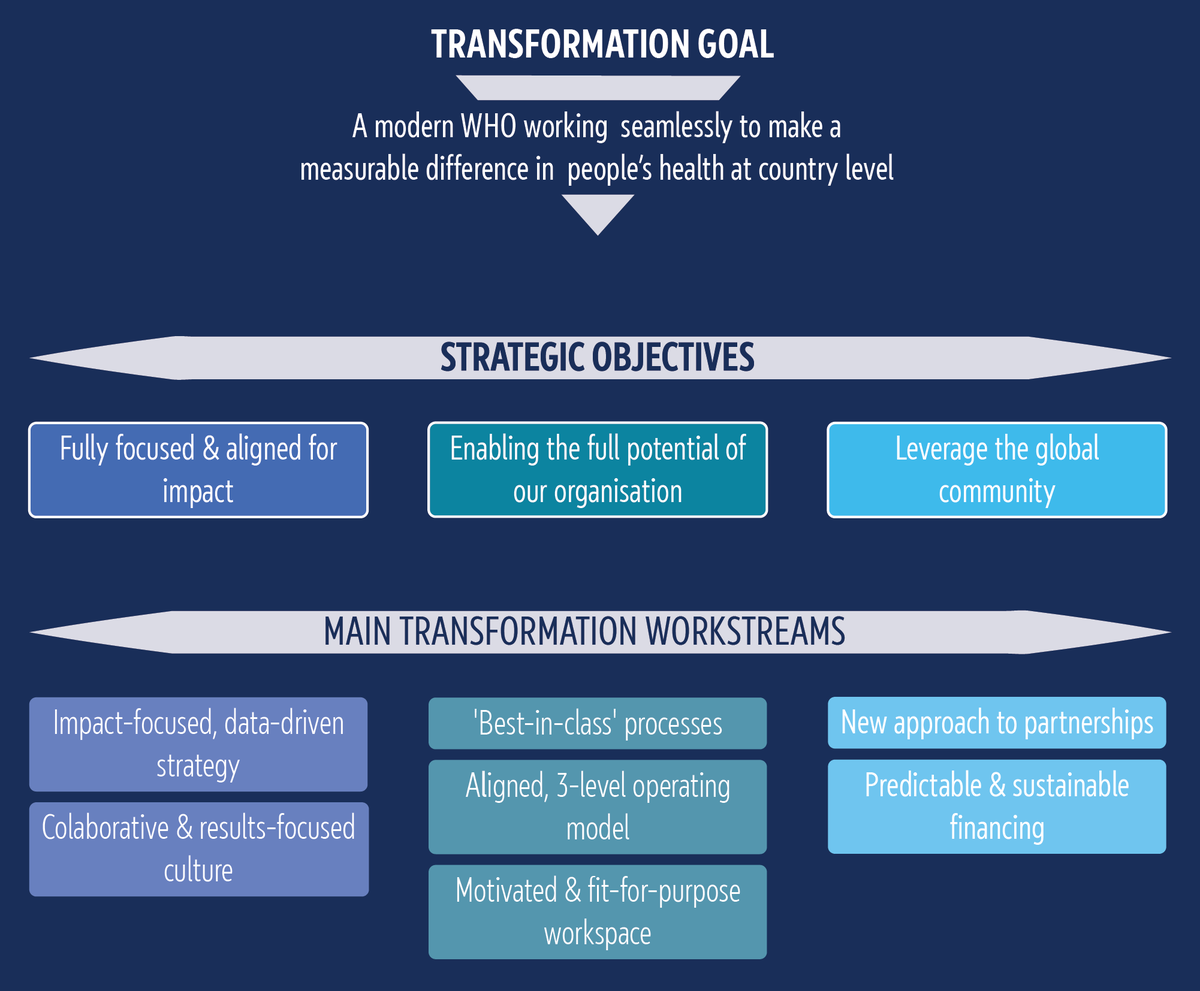
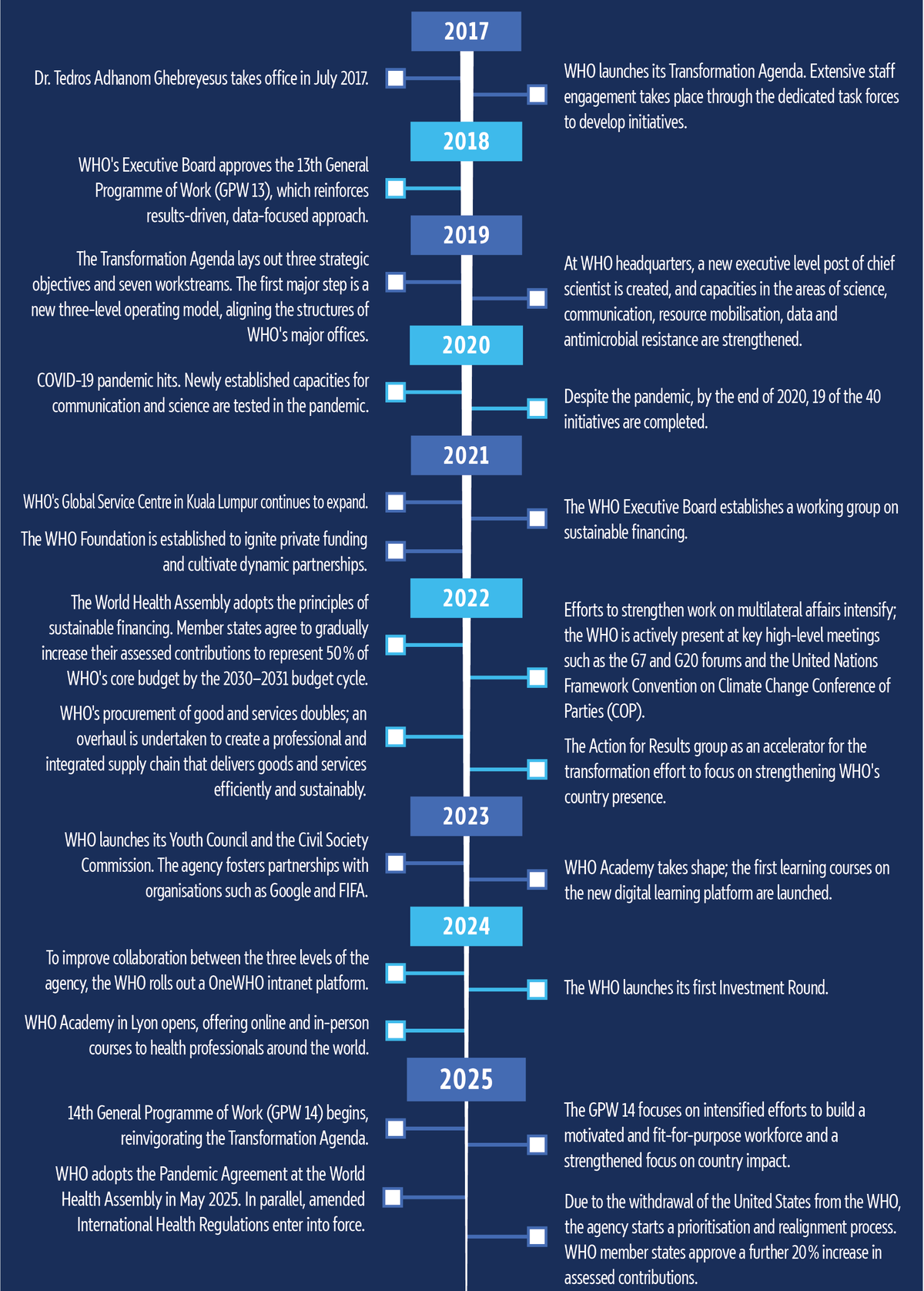
To address key shortcomings and increase its capacity to overcome evolving challenges, the WHO launched its Transformation Agenda almost 10 years ago, in July 2017. The WHO Transformation Agenda is centred on three strategic objectives, advanced through the transformation workstreams (see Figure 5). The first objective is to ensure that the agency is fully focused and aligned for impact at the country level. The second objective is to allow the agency to reach its full potential to provide authoritative advice and leadership on critical health matters in a rapidly changing environment. The third objective is to leverage partnerships to fully engage the global community. Currently, the Fourteenth General Programme of Work (GPW 14), developed based on lessons learned from the COVID-19 pandemic and evaluation of the Thirteenth General Programme of Work, builds on the first six years of the Transformation Agenda, and continues to steer the transformation (see Figure 6).
Source: Compiled by the author, based on WHO data. Graphic by Nadejda Kresnichka-Nikolchova, EPRS.
Source: Compiled by the author, based on WHO data. Graphic by Nadejda Kresnichka-Nikolchova, EPRS.
EU and WHO
Since early 1970s when the WHO and the European Commission started their technical cooperation, the EU has formed a long-lasting strategic partnership with the agency. Currently, the cooperation between the EU, represented by the European Commission, and the WHO is based on an exchange of letters from 2001, which sets out general principles, objectives and procedures for the cooperation. EU–WHO strategic cooperation was extended in December 2022, when the partners reaffirmed their commitment to enhance strategic cooperation in global health security and architecture, and to cooperate on the implementation of major initiatives and shared EU and WHO priorities.
EU global health strategy
The 2022 EU global health strategy (EU GHS) underlines that 'WHO is the indispensable cornerstone of the multilateral health system'. Therefore, the strategy guides the EU and its Member States to ensure further strengthening of the WHO's leadership, effectiveness, efficiency and accountability, and align EU and WHO priorities.
The EU GHS outlines the following lines of action to be prioritised:
-
seek formal EU observer status with full participation rights as a first step towards full WHO membership;
-
contribute to making the financing of WHO more sustainable by 2030-2031;
-
advance WHO reform to strengthen its governance, efficiency, accountability and enforcement of rules, in accordance with its member-driven nature;
-
strengthen the WHO's focus on its normative role in areas of global relevance;
-
enhance cooperation with the WHO at central and regional European level to ensure greater alignment of EU and WHO priorities.
In May 2026, the Commission adopted a communication on reinforcing global health resilience amidst geopolitical change. It reiterated the EU support for a global health architecture with the WHO, focused on its core normative, standard-setting, global health security, and coordination and convening mandates at its centre.
The EU and the WHO cooperate at three geographic levels:
-
with the WHO headquarters in Geneva, on issues of global concern, where EU–WHO top common priorities are : (i) health systems strengthening and UHC; (ii) access to medicines; (iii) health emergencies and humanitarian aid; (iv) global health security; (v) One Health and antimicrobial resistance; and (vi) health determinants;
-
with the WHO Regional Office for Europe on European issues; in 2020, the partners renewed the commitment to work together to strengthen cooperation on health security, health systems, NCDs with a focus on cancer, sustainable food systems, and cooperation with non-EU countries;
-
with separate countries (country-level cooperation).
Financially, the EU and its Member States stand as the WHO's foremost contributors. The EU backed the 2024 WHO Investment Round with over €250 million from the Commission, while Team Europe pledged US$783 million (almost €690 million) for the 2025-2028 period. Under the EU4Health programme alone, €92.68 million was allocated between 2021 and 2024 through contribution agreements and direct grants with the WHO. Of this amount, €56 million supports crisis preparedness; over €11 million is dedicated to health promotion and disease prevention; and more than €10 million is allocated to cancer-related initiatives. Additionally, €9.5 million is directed towards health systems and workforce-related projects.
Beyond funding, the EU (Commission's services and the European External Action Service (EEAS)) engage with the WHO at strategic, diplomatic, technical and operational levels, including via the EU Delegation in Geneva. The Commission participates as an observer in annual meetings of the WHO Executive Board and the World Health Assembly, as well as in the annual meetings of the WHO Regional Committee for Europe. Moreover, the Commission and the EEAS coordinate with the EU Member States ahead of key WHO meetings, such as the World Health Assembly, Executive Boards meetings and regional committee meetings, notably to prepare joint statements and negotiate texts. To give an example, the Commission was closely involved in negotiations on the WHO Framework Convention on Tobacco Control (FCTC), developed under the auspices of the WHO, and supports its implementation. Most recent EU governance contributions include EU-led amendments to the International Health Regulations (2024) and WHO Pandemic Agreement (2025). The EU also maintains regular high-level strategic meetings with WHO leadership.
All relevant Commission services6 and EU agencies7 are involved in the cooperation. For instance, the European Agency for Safety and Health at Work (EU-OSHA) and European Centre for Disease Prevention and Control (ECDC) partnerships with the WHO address occupational hazards and disease elimination goals respectively. On the ground, deployments to Africa Centres for Disease Control and Prevention (Africa CDC) and to mpox responses exemplify tangible impacts, ensuring equitable global health security.
Selected examples of EU–WHO cooperation
The EU, through the Commission, also supports a wide range of WHO programmes, focusing on areas such as UHC, health systems strengthening worldwide, health security, antimicrobial resistance, enhancing laboratory capacities in Africa, advancing wastewater surveillance for public health and the intersection of health and environmental issues, as well as on strengthening health information systems in Europe and globally.
Universal health coverage partnership
In 2011, to promote UHC at country level through strengthening health systems, the WHO and the EU initiated the universal health coverage partnership (UHC partnership).8 With a focus on NCDs, health security, gender, equity and human rights, the partnership supports countries to achieve UHC through a primary health care approach. It focuses on (i) access to medicines, vaccines and health products; (ii) governance and strategic planning; (iii) health financing; (iv) health information; (v) service delivery; and (vi) health workforce. In particular, through the deployment of more than 145 health policy advisors in 125 countries with a population of over 3 billion people, the partnership supports their ministries of health in an evidence-based and inclusive policymaking process, from the development and strengthening of country health plans and policies, to their effective implementation. Between 2011 and 2019, this partnership helped to increase the global average UHC of essential health services by 10 percentage points: from 58 % to 68 %. Against the backdrop of stalling progress amid the COVID-19 pandemic, in November 2022, the EU committed to investing an additional €125 million during the 2023-2027 period. This contribution made the EU the largest donor to the UHC partnership, which itself is a key deliverable of the EU GHS.
Cooperation in health emergencies
The EU and WHO cooperate in the field of humanitarian response. The EU, through the European Commission's Directorate General for Civil Protection and Humanitarian Aid Operations (DG ECHO) and other relevant services, contribute to global health security by supporting the outbreak and crisis response operations of the WHO health emergencies programme worldwide. Together, the WHO and the EU provide humanitarian relief and assistance to the communities affected by health emergencies in Afghanistan, the Democratic Republic of the Congo, Iraq, Lebanon, Nigeria, South Sudan, Syria, Ukraine, Yemen, and other countries.
The EU–WHO partnership focuses on both financial and operational support. The partners cooperate, in particular, through the Global Health Cluster, sharing best practice, promoting preparedness and response, and supporting health resilience. As for the operational part, the EU coordinates its action with the WHO to support its emergency medical teams, mobilised by the European Medical Corps under the European Civil Protection Pool, a part of the Union Civil Protection Mechanism to provide direct medical care to people affected by a disaster. This cooperation between the EU and the WHO contributes to the reduction of loss of life and the prevention of long-term disability as a result of disasters, outbreaks and other emergencies.
Cooperation on global health security
Strengthening global health security is one of the shared priorities of the EU and the WHO. In December 2022, the European Commission's Health Emergency Preparedness Authority (HERA) and the WHO launched a partnership for stronger pandemic preparedness and response. With a €15 million allocation under the EU4Health programme, the actions focus on providing information, capacities and tools against health emergencies with the aim of strengthening global capacities. In particular, HERA funds the following key global initiatives:
-
assisting decisionmaking concerning health emergencies preparedness and response through the WHO Hub for Pandemic and Epidemic Preparedness;
-
the development of new medical countermeasures for tackling anti-microbial resistance (AMR); this initiative also aims to ensure sustainable access to and affordability and responsible use of AMR treatments;
-
the scaling up of national capacities for SARS-CoV-2, emerging pathogens detection, and genomic surveillance in Africa;
-
the COVID-19 technology access pool (C-TAP).
In addition, in December 2025, the WHO and HERA signed a €3.5 million agreement to expand their partnership to combat antimicrobial resistance under the EU4Health programme. This is to support WHO in monitoring the development of antimicrobials and medical countermeasures, developing guidelines for new antibacterial innovations, and implementing WHO priority pathogen lists to guide research and public health efforts.
In parallel, in the framework of the Global Health Security Initiative (GHSI),9 the EU – through the European Commission – works closely with the WHO, as well as with Canada, France, Germany, Italy, Japan, Mexico, the UK and the US, to strengthen public health preparedness and response globally to health threats.
European Parliament position
The European Parliament is a vocal supporter of more proactive action on global health. In various resolutions (see text box with examples below), Parliament expressed its support to the agency and called on the Commission and the EU Member States to comply with various WHO measures, initiatives and guidelines.
Examples of the European Parliament's stance on the WHO
In its resolution of 9 July 2025 on implementation and delivery of the Sustainable Development Goals (SDGs) in view of the 2025 High-Level Political Forum, the European Parliament stressed that 'health threats know no borders and that a local health emergency can quickly escalate into a global pandemic, necessitating a coordinated global response and strengthened international cooperation through robust multilateral health institutions, in particular WHO'. In this resolution, the Members of the European Parliament (MEPs) expressed their deep regret about the US decision to withdraw from the WHO, stressing that 'this withdrawal will significantly hinder progress towards achieving SDG 3 by reducing capacities for monitoring health threats, as well as international coordination, resources and leadership in addressing health crises and promoting equitable access to health for all'.
Parliament's resolution of 12 July 2023 on the COVID-19 pandemic underlined the need to further reinforce the cooperation between the EU and the WHO with a more coordinated, long-term approach, and with a stronger, well-funded and independent UN. The resolution called for the EU to promote the reinforcement and expansion of the WHO by increasing its overall budget and reinforcing its work on potential exposure routes and the highest-risk environments for transmission of zoonotic diseases. This resolution also stressed the need for the EU to assume the role of a formal observer at the WHO.
Other resolutions on specific health-related topics called on the EU institutions and the Member States to comply with WHO measures. For instance, Parliament's resolution of 1 June 2023 on EU action to combat antimicrobial resistance called on the Member States and the Commission to support WHO initiatives to prepare guidance on how good manufacturing practices should be implemented to waste and waste-water management in the context of the production of antimicrobials. In its resolution of 13 December 2023 on non-communicable diseases, Parliament called on the Commission and the Member States to contribute to the implementation of the 2019 WHO resolution on improving the transparency of markets for medicines, vaccines and other health products. In parallel, through Parliament's resolution of 12 December 2023 on mental health, MEPs called on the Commission and the Member States to implement WHO evidence-based interventions in suicide-prevention programmes. Amid the COVID-19 pandemic, Parliament's resolution of 10 July 2020 on the EU's public health strategy post-COVID-19 called on the EU to cooperate fully with WHO and other international bodies to combat infectious diseases, achieve universal health coverage for all, and strengthen health systems globally.
Endnotes
Classification
Policy areas: Public Health | Global Governance
Regions: Asia and Pacific, Canada and United States, Central Asia, European Union, Latin America and Caribbean, Mediterranean and Middle East, RUSSIA, Non-EU Europe and the North, Sub-Saharan Africa
Committees: Environment, Climate and Food Safety (ENVI)
Disclaimer
This document is prepared for, and addressed to, the Members and staff of the European Parliament as background material to assist them in their parliamentary work. The content of the document is the sole responsibility of its author(s) and any opinions expressed herein should not be taken to represent an official position of the Parliament.
Copyright
© European Union.
The reuse of this document is authorised under a Creative Commons Attribution 4.0 International (CC-BY 4.0) licence.

https://creativecommons.org/licenses/by/4.0/deed.en
To use or reproduce elements that are not owned by the European Union, permission may need to be sought directly from the respective rightsholders.